
Phase I, II, and III Trials: What Each Actually Tests
Clinical trials happen in phases for a reason. An exploration of what Phase I, II, and III trials are designed to test—and what early results cannot yet establish.

What "in trials" actually tells us
News coverage of medical research often treats clinical trial phases as a simple ladder: Phase I, then Phase II, then Phase III. Each step is often portrayed as stronger proof that a treatment works.
But the phases of clinical trials are not simply three rounds of the same test with large sample sizes. Each phase asks a different scientific question, using different populations, study designs, and endpoints. A Phase I result and a Phase III result are not comparable pieces of evidence—but they are regularly reported with similar confidence.
Understanding what each phase is actually designed to test helps explain several patterns in research: why early trial results often change later, why many promising treatments fail in Phase III, and why headlines about early findings frequently overstate what has been demonstrated.
Why trials happen in phases at all
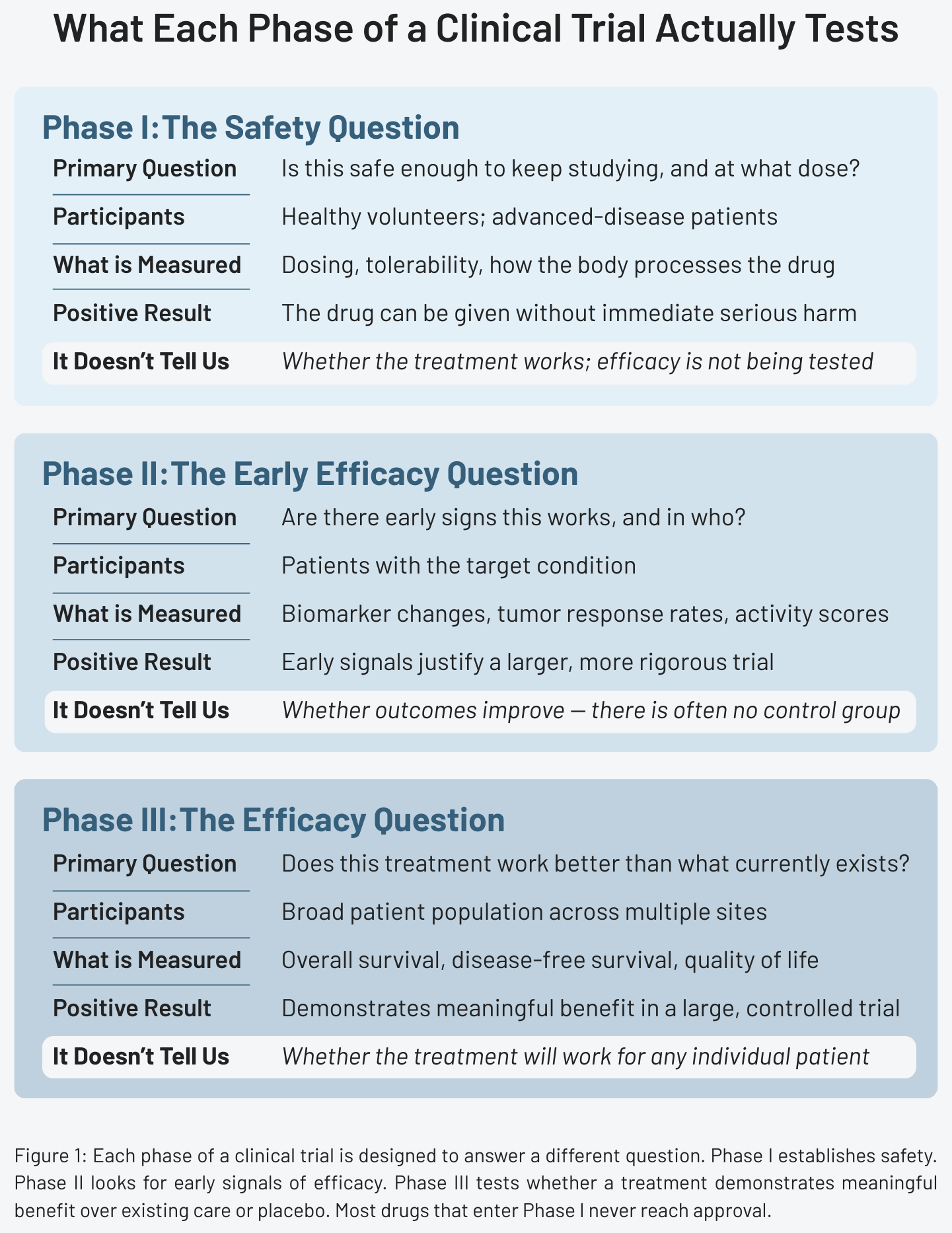
The staged structure of clinical trials exists to manage risk. You can’t test whether a new treatment is effective in thousands of patients before first establishing that it isn’t immediately harmful. Each phase gates entry to the next and each is designed to answer progressively more demanding questions about safety and, eventually, efficacy.
The pipeline is also highly attritive. Roughly 90% of drugs that enter clinical trials fail to reach regulatory approval. Most are eliminated somewhere in the process because they cause unacceptable side effects, because early efficacy signals don’t hold up under rigorous testing, or because they work no better than what already exists.
“In trials” is not close to “approved.” It’s the beginning of a long, uncertain process in which failure is far more common than success.
If you want a simple framework for evaluating new health studies in the news, subscribers receive a free guide: 5 Questions to Ask Before Believing a Health Headline
Phase I — the safety question
Phase I trials represent the first time a new treatment is tested in people. The primary question is narrow: is this safe enough to keep studying, and at what dose?
These trials typically enroll small groups—often between 20 and 100 participants—using a dose-escalation design. Researchers start at a low dose, monitor closely for adverse effects, and increase incrementally until they identify either a therapeutic range or a level of toxicity that limits further escalation. The goal is to determine the maximum tolerated dose and to characterize how the body processes the drug—how it’s absorbed, distributed, metabolized, and eliminated.
Who participates depends on the therapeutic area. In most fields, Phase I trials recruit healthy volunteers. In oncology, where experimental treatments often carry significant risks and the potential benefit may justify those risks, participants are typically patients with advanced disease who have exhausted standard treatment options.
Phase I trials are not designed to measure clinical effectiveness. They are typically too small and too short to reliably detect improvements in health outcomes. There is no comparison group and no placebo. Researchers are focused on determining whether the drug can be given to a human being without causing immediate serious harm.
A positive Phase I result means exactly that: the treatment can be administered at a testable dose without unacceptable toxicity in a small group of participants. That is a meaningful prerequisite for further research. It is not evidence that the treatment is effective.
When headlines describe a drug as having "completed Phase I successfully," that is the threshold being reported.
Phase II — the early efficacy question
If a treatment appears reasonably safe in Phase I, the next question is whether there are early signs it might work–and in which patients.
Phase II trials are larger, typically enrolling between 100 and 500 participants, and are focused on a more specific population than Phase I. The question shifts from safety toward preliminary efficacy: does the treatment produce measurable biological or clinical changes in the people it's intended to help?
What Phase II measures is often intermediate. Researchers track tumor response rates, biomarker changes, disease activity scores, or other signals that suggest the treatment is doing something. These are not the same as outcomes that matter directly to patients—survival, quality of life, symptom relief over time—but they can indicate whether a treatment is biologically active and worth studying further.
A critical structural limitation shapes what Phase II can actually tell us: many Phase II trials do not include a control group. Participants receive the experimental treatment, and their outcomes are tracked—but there is no comparison arm receiving standard care or a placebo. Without a control group, it’s difficult to know how much of any observed change reflects the treatment versus the natural course of the disease or the placebo effect. A tumor that responds during a Phase II trial may have responded for reasons unrelated to the drug being studied.
This is also where many of the findings that generate headlines originate. A response rate in a Phase II trial—"60% of patients saw tumor reduction"—can sound compelling in isolation. Without knowing what response rates look like in similar patients receiving standard care, that number carries limited interpretive weight. It is a signal, not a conclusion.
A positive Phase II result means there are early signs worth investigating in a larger, more rigorous trial. It justifies proceeding. It does not establish that the treatment works.
Phase III — the efficacy question
Phase III is where the central question of drug development is finally asked: does this treatment work as well as or better than what currently exists, in a large and representative population?
Phase III trials are substantially larger than earlier phases—often enrolling hundreds to thousands of participants across multiple sites. They are typically randomized and controlled, meaning participants are assigned by chance to receive either the new treatment or a comparator, usually the current standard of care or a placebo when no standard care exists. Many Phase III trials are also blinded: participants don't know which treatment they're receiving, and in double-blind designs, neither do the clinicians administering it. These features are designed to reduce bias and isolate the treatment's true effect.
What Phase III measures are outcomes that matter to patients: overall survival, disease-free survival, quality of life, rates of recurrence, and time to disease progression. These are not intermediate signals or biological markers—they are the endpoints that determine whether a treatment improves how long or how well patients live.
This is also where most drugs fail. Phase III exposes the gap between early promise and real-world benefit. A treatment can show compelling Phase II response rates and still fail to extend survival in a Phase III trial. It can reduce a biomarker reliably and still not improve patient outcomes. The reasons vary: the early signals may not have reflected the mechanisms that actually drive patient benefit, the Phase II population may have been more selected than the broader Phase III group, or comparison against standard care reveals that the treatment's advantage is smaller than preliminary data suggested.
Regulatory approval in most countries requires at least one successful Phase III trial demonstrating meaningful benefit over existing options. This is the evidentiary standard the public rarely hears described explicitly—and it is considerably more demanding than anything Phase I or Phase II requires. When a treatment is approved, it has cleared this bar. When a treatment is "in trials," it has not yet been asked to.
How to read trial headlines more carefully
When you encounter a headline describing a drug as promising or advancing through clinical testing, a few questions help clarify what the evidence actually shows:
- What phase is this?
- Was there a control group?
- What endpoint was measured—a biomarker or response rate, or a patient outcome like survival or quality of life?
- How many participants were enrolled and how similar are they to the broader population this treatment would eventually serve?
- Has the finding been replicated in independent trials, or does the evidence rest on a single study?
Why this matters
Clinical trial phases are often presented as simple milestones. In reality, they reflect a broader principle of scientific research: strong conclusions require progressively stronger tests.
"In trials" can describe a drug in its first small safety experiment or one under regulatory review after a successful Phase III program. The phrase carries no information about where in the pipeline the evidence sits, or how demanding the testing has been. For patients and families following research relevant to a diagnosis, that distinction matters. Phase I results represent a hypothesis being safely explored—not a treatment approaching clinical availability. Phase II signals are worth tracking, but they have a long history of failing to survive the more rigorous demands of Phase III.
The staged structure exists because medicine has learned, sometimes slowly and at cost, that early promise is an unreliable predictor of final benefit. Most drugs don't make it through. The ones that do have been asked increasingly difficult questions at each stage and have answered them well enough to keep advancing.
Understanding what each phase actually measures doesn't make early trial results less interesting. It makes them easier to interpret accurately—as one step in a long process, not as evidence of something already proven.
References
- Clinical Trial Phases, National Cancer Institute
- Clinical Trials and Clinical Research: A Comprehensive Review, Cureus
- Advancing Drug Safety in Drug Development, Chemical Research in Toxicology
- FDA Acceptance of Surrogate End Points for Cancer Drug Approval: 1992-2019, JAMA Internal Medicine
- Factors associated with clinical trials that fail and opportunities for improving the likelihood of success, Contemporary Clinical Trials Communication