
What “Cancer Breakthrough” Usually Means in Early Research
Headlines declare cancer breakthroughs regularly. Most of them describe findings that are years—or decades—away from helping patients. A closer look at what early-stage cancer research actually shows, and what gets lost in translation.

Why ‘breakthrough’ language is everywhere in cancer coverage
Cancer is one of the most emotionally charged subjects in medicine. It affects nearly everyone—directly or through a loved one—and has been the focus of public optimism and frustration for decades. As a result, media coverage of cancer is rarely neutral. Hope, urgency, and the sense that progress must be just around the corner often influence reporting before readers encounter a single piece of data.
‘Breakthrough’ is one of the most common words in that coverage. The problem is that it has no standardized scientific meaning. It might describe a discovery that fundamentally changes our understanding of cancer biology. It might also describe a single experiment in which cancer cells were killed in a petri dish. Both uses appear in mainstream reporting with similar confidence, and without additional context, readers have almost no way to distinguish between them.
This isn’t purely a journalism problem. Research institutions issue press releases that frame early findings optimistically. Scientists sometimes use enthusiastic language when discussing results. Funding cycles and competitive pressures create incentives to signal progress. And audiences gravitate toward stories that suggest answers are close. The result is a feedback loop in which early-stage findings are routinely framed as near-term solutions.
Understanding what early cancer research can—and cannot—show requires stepping back from headline language and looking at how research actually progresses.
Types of early cancer research
Cancer research moves through a structured pipeline. Where a finding sits in that pipeline determines what it actually tells us. Most ‘breakthrough’ headlines describe findings from the very beginning of that process—not the end.
In vitro studies
The earliest phase of cancer research often takes place in a petri dish. Researchers expose cancer cells—grown in a controlled laboratory environment—to a compound, treatment, or genetic intervention and observe what happens. They measure outcomes such as cell death, growth rate, or molecular changes.
These studies are essential for understanding mechanisms. But cancer in a dish is not cancer in a human body. Tumors exist within complex biological environments—blood supply, immune cells, signaling pathways, metabolism—that can dramatically change how a treatment behaves. Many substances kill cancer cells in vitro, including ones that would be toxic or ineffective in a person.
An in vitro result is a starting point, not a treatment.
Animal studies
If a cell study looks promising, the next step often involves testing in animals, typically mice. Animal studies add biological complexity: a living immune system, circulation, metabolism, and organ interactions.
They can help determine whether a treatment appears safe enough to justify human testing and whether the biological mechanism observed in cells operates in a living organism. But animal models have significant limitations, especially in oncology. Tumors in mice are often induced rapidly and can behave differently than slow-growing, genetically diverse cancers that develop in humans.
A long track record of promising mouse results that failed in human trials reflects this gap. Success in animals is a reason to proceed cautiously, not proof of effectiveness in people.
Phase I clinical trials
The first time a new intervention is tested in humans, safety is the primary concern. Phase I trials typically involve small numbers of participants—often patients with advanced disease who have exhausted other options. These studies are designed to establish dosing and identify serious side effects.
A positive Phase I result confirms that a treatment can be administered without causing immediate serious harm. It does not demonstrate that the treatment works.
Phase II clinical trials
Phase II trials are larger and begin to evaluate whether a treatment shows signs of efficacy. Researchers may report tumor response rates or other early indicators of benefit.
A treatment that performs well in Phase II can generate significant excitement. But these results are still preliminary. Many therapies that look encouraging at this stage fail to demonstrate meaningful benefit when tested in larger, more rigorous trials.
Phase III clinical trials
Phase III trials compare a new treatment to the current standard of care in large, often randomized groups of patients. This is where the most robust evidence is generated, and where many drugs that looked encouraging earlier fail to demonstrate meaningful advantage.
Regulatory approval typically requires at least one successful Phase III trial. This stage is most closely associated with genuine, evidence-supported progress. It is also the stage most likely to reveal that earlier optimism was premature.
Most headlines declaring a cancer breakthrough describe findings from the first two stages of this pipeline—before any human has received the treatment or before it has been rigorously compared to existing care.
If you want a faster way to read health studies without oversimplifying them, subscribers get a free guide: How to Read a Health Study in 10 Minutes.
What ‘breakthrough’ often actually means
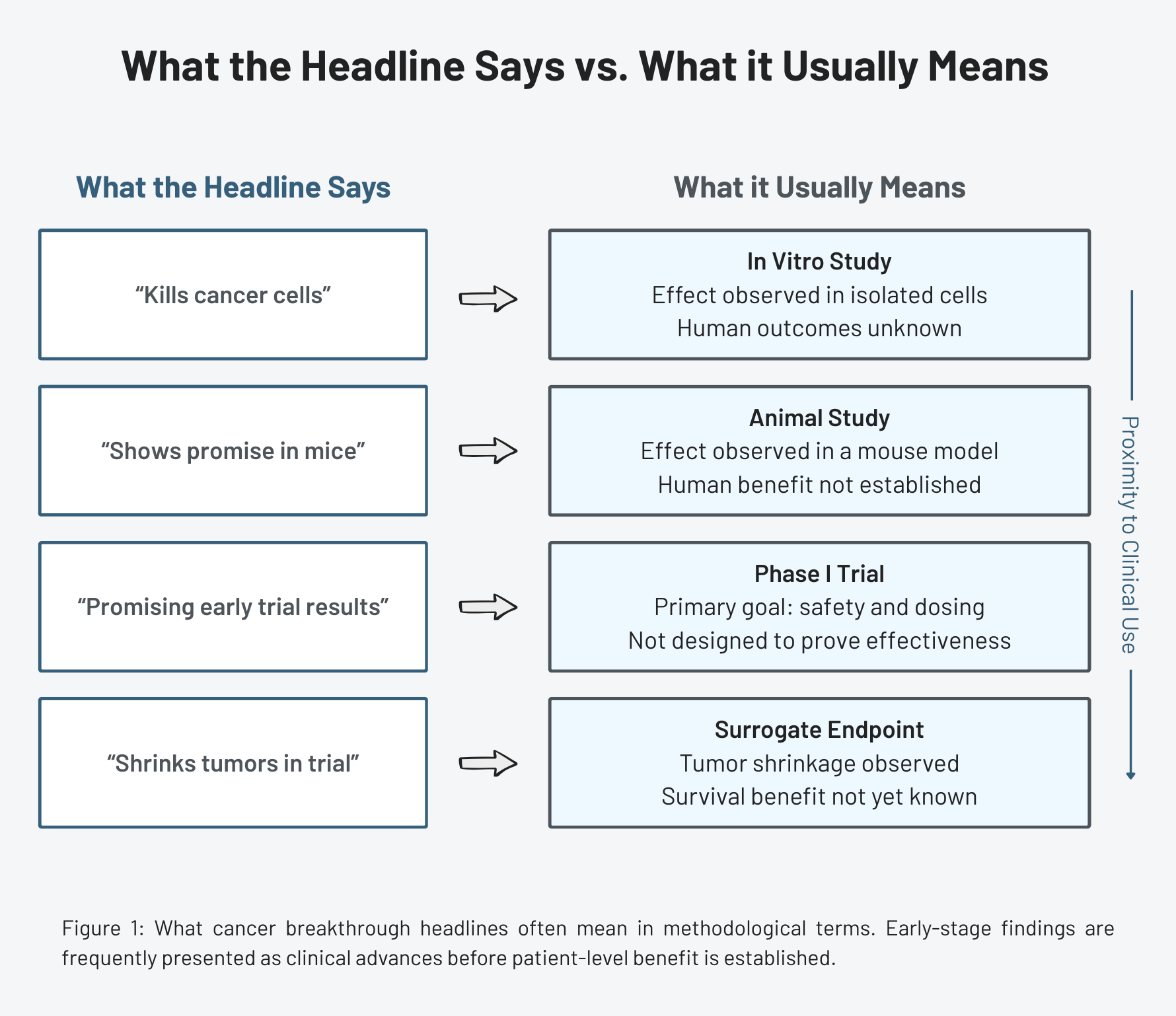
When you map headline language onto the research pipeline, a pattern emerges: the words used in media coverage often outpace the evidence.
Kills cancer cells
When a headline says a compound ‘kills cancer cells,’ it almost always refers to an in vitro finding. Something destroyed cancer cells in a dish.
This may be scientifically interesting, especially when it points to a novel mechanism. But it describes an early observation, not a therapy. The gap between ‘kills cancer cells in a lab’ and ‘works as a cancer treatment’ is enormous and typically involves years of additional research with uncertain outcomes.
Promising in mice
When a headline reports that a treatment ‘shows promise in mice,’ it describes a preclinical finding. The intervention worked in an animal model under controlled conditions.
This moves a finding one step closer to human testing, but the translation rate from animal cancer research to approved human therapies is very low. A result that works in mice is a hypothesis worth testing in people, but it’s not evidence that it will work in people.
Biomarker changes
Another common source of headlines is a change in a biological marker—a protein level, a gene expression pattern, or an immune signal.
Biomarkers can help provide valuable insight into how a treatment works and may help predict response, but a change in a biomarker does not automatically translate to a change in patient outcomes. A therapy may normalize a lab value without affecting survival, symptoms, or quality of life.
Tumor shrinkage in early trials
A frequent scenario in early trial coverage: a new drug produces measurable tumor shrinkage in a subset of patients.
Tumor response is a meaningful signal, but it’s not the same as a survival benefit. A treatment can shrink tumors without extending life or improving quality of life. The more consequential question—did patients live longer?—often requires longer follow-up to answer.
None of this means early-stage findings are unimportant. Every approved cancer therapy began as a hypothesis tested in cells or animals. The problem isn’t the early research, it’s that the early research is routinely described using language that implies it has already crossed finish lines it has barely approached.
Why legitimate findings get amplified beyond their evidence
If the underlying science is often careful and qualified, why does the public message become so inflated?
The gap between what early research shows and how it gets reported reflects structural incentives—not simply scientific illiteracy.
Media outlets compete for attention. Journalists face time pressure and audience expectations. Even well-intentioned reporters covering a complex field may not have the background to independently evaluate a preclinical claim. Editors may sharpen headlines in ways that remove nuance. Coverage may accurately summarize a press release while failing to accurately represent the strength of the underlying evidence.
Universities and research institutions also operate within competitive environments. Funding, prestige, and public visibility matter. Even when researchers themselves are cautious in their language, institutional reporting may emphasize potential impact. The cautious tone of scientific writing rarely survives translation into public communication.
Patients and advocates add another layer. The demand for hope in the face of serious illness is real and understandable. Stories that suggest progress—even if preliminary—meet a genuine psychological need, and that demand further rewards optimistic framing.
These dynamics are systemic. Early findings in science are often the most dramatic. Over time, further research gradually refines, qualifies, or sometimes contradicts those initial results. But headlines tend to capture only the first spike of excitement.
How to read a cancer research headline more carefully
When you encounter the next ‘cancer breakthrough,’ a few questions can clarify what you’re actually looking at:
- What stage of research is this? (Cell study? Animal study? Phase I, II, or III trial?)
- If it has been tested in humans, how many participants were involved?
- What endpoint was measured—tumor response, biomarker change, progression-free survival, or overall survival?
- Was the new treatment compared to standard care?
- Has the finding been independently replicated?
Asking these questions can help place findings in context. Early research is meant to be exploratory. It generates hypotheses, identifies promising targets, and justifies larger trials. It is not designed to deliver final answers.
Why this matters
Overstating early cancer research has consequences.
When preliminary findings are presented as near-term solutions, patients and families may form expectations that don’t align with the reality of treatment development. Some may pursue experimental options based on limited evidence rather than established therapies with stronger support. Hope grounded in a misunderstanding of what the research actually shows can lead to harmful decisions.
At a broader level, repeated cycles of hype and disappointment can fuel skepticism about medical research itself. When widely publicized breakthroughs fail to materialize, it can erode trust in the findings that do hold up.
None of this is an argument against reporting on early cancer research. Oncology has seen genuine breakthroughs: targeted therapies, immunotherapies, and meaningfully extended survival for many patients. But those successes emerged through years of incremental work, replication, and large-scale trials.
Understanding what a ‘breakthrough’ finding actually shows—where it sits in the research process, and what would need to happen before it changes clinical care—helps align hope with evidence.
Learning to interpret cancer research more carefully doesn’t dampen optimism. It grounds it in the reality of how science advances.
References
- Raise standards for preclinical cancer research, Nature
- The Strength of Association Between Surrogate End Points and Survival in Oncology, JAMA Internal Medicine
- High drug attrition rates—where are we going wrong?, Nature Reviews Clinical Oncology
- Analysis of animal-to-human translation shows that only 5% of animal-tested therapeutic interventions obtain regulatory approval for human applications, PLOS Biology
- Estimated Research and Development Investment Needed to Bring a New Medicine to Market, 2009-2018, JAMA